When Cells Become Drugs: The Rise of Allogeneic CAR-T
Cancer treatment has traditionally relied on surgery, radiation, and drugs. CAR-T therapy introduced something entirely different: using living cells as medicine.
In CAR-T therapy, a patient's own immune cells are collected, genetically reprogrammed, expanded in the laboratory, and then returned to the body to hunt down cancer cells. For some patients with blood cancers, the results have been remarkable, producing remissions that were once considered unlikely.
But CAR-T therapy also reveals a fascinating question: if living cells can be medicines, can we manufacture them like medicines too?
That question is driving the development of allogeneic CAR-T, one of the most ambitious areas in modern biotechnology.
Teaching Immune Cells New Tricks
To understand CAR-T therapy, it helps to start with how T cells normally work.
T cells are the immune system's professional inspectors. They constantly patrol the body, checking other cells for signs of infection or disease. They do this by recognizing small protein fragments, called antigens, displayed on the cell surface.
When a T cell recognizes a dangerous antigen, it becomes activated and destroys the abnormal cell.
Cancer, however, is a master of disguise. Tumor cells can hide from the immune system by reducing antigen presentation or suppressing immune responses. As a result, many cancer cells escape detection.
CAR-T therapy bypasses this problem.
Scientists genetically engineer T cells to produce a synthetic receptor called a Chimeric Antigen Receptor (CAR). This receptor allows the T cell to recognize specific proteins on the surface of cancer cells directly, without relying on the usual immune recognition pathways.
A CAR contains three main parts:
An external binding region that recognizes a tumor marker such as CD19 or BCMA
A membrane anchor that holds the receptor in place
Internal signaling domains that activate the T cell when the target is detected
When a CAR-T cell encounters a cancer cell carrying its target, it becomes activated, multiplies rapidly, and releases toxic molecules that kill the tumor cell. Afterward, it can move on and attack additional cancer cells.
In simple terms, scientists have turned a naturally occurring immune cell into a programmable cancer-fighting machine.
From Personalized Cell Therapy to Off-the-Shelf CAR-T
Today's approved CAR-T therapies are mostly autologous, meaning they are made from the patient's own cells. This process is highly personalized. Doctors collect T cells from the patient, send them to a manufacturing facility, genetically modify them, grow millions of copies, perform quality testing, and finally ship them back for treatment.
This approach works, but it comes with challenges. Manufacturing can take several weeks. Some patients become too sick while waiting. Others may not have enough healthy T cells to produce an effective therapy. Because every treatment starts with a different patient, every batch is slightly different. The process resembles a custom medical procedure more than a traditional drug.
Allogeneic CAR-T takes a completely different approach. Instead of using the patient's cells, scientists begin with T cells collected from healthy donors. These cells are engineered in advance, expanded into large batches, frozen, and stored until needed.
Rather than creating one treatment for one patient, a single manufacturing run can potentially generate treatments for many patients. That is the promise of allogeneic CAR-T.
Potential advantages include:
Faster treatment availability
More consistent product quality
Reduced manufacturing costs
Greater accessibility for patients
More importantly, it represents a shift in how we think about cell therapy. Instead of a personalized procedure, the therapy starts to resemble a conventional pharmaceutical product—it can be manufactured, stocked, and delivered on demand.
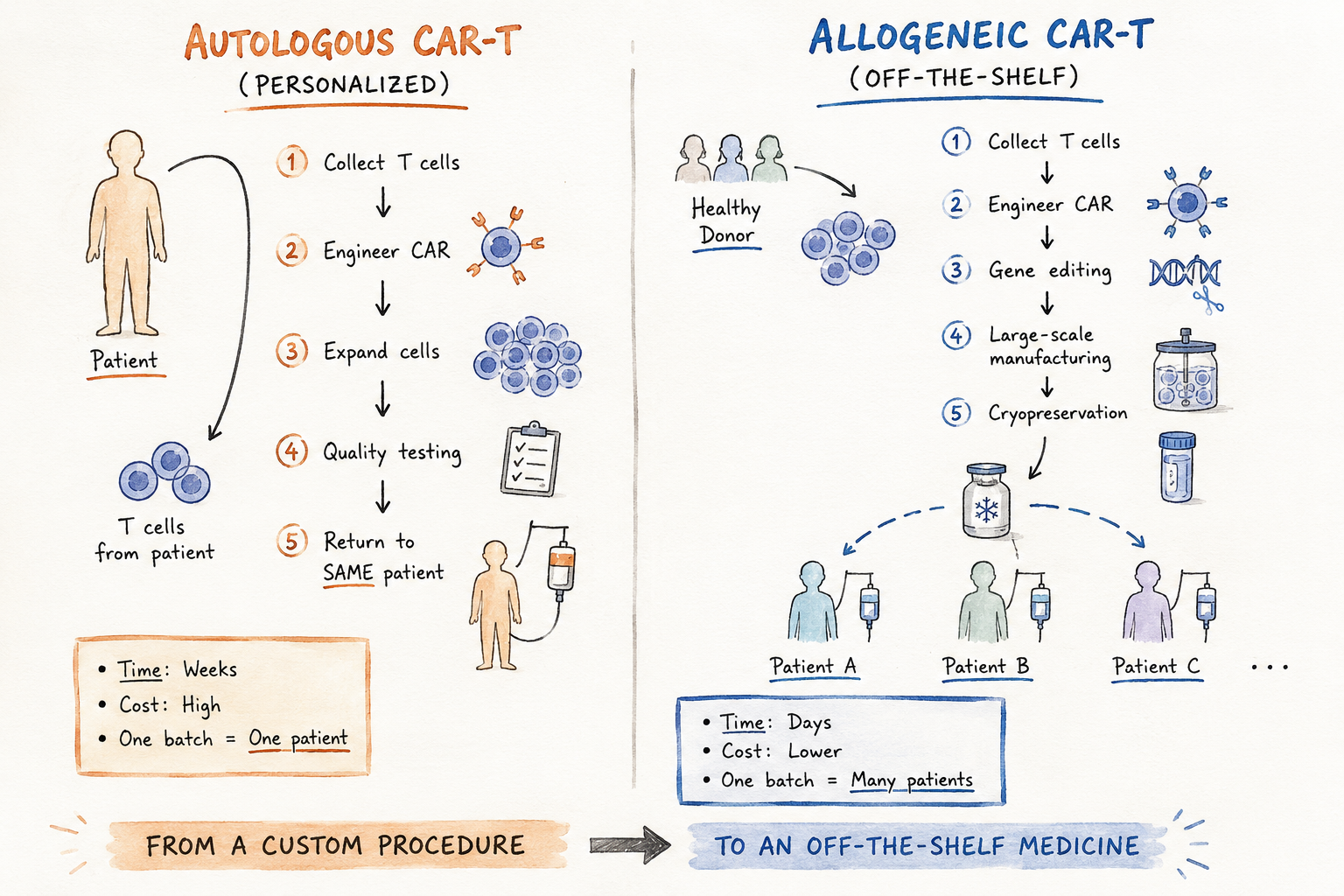
Comparison of autologous and allogeneic CAR-T cell therapy. In autologous CAR-T, T cells are collected from an individual patient, engineered to express a CAR, expanded, tested, and returned to the same patient. In allogeneic CAR-T, T cells from a healthy donor are engineered, gene-edited, manufactured at scale, cryopreserved, and stored for use in multiple patients as an off-the-shelf therapy. AI-generated illustration created with author guidance and reviewed for scientific accuracy.
The Immune System Fights Back
The idea sounds simple, but the biology is not. Our immune system is designed to distinguish between "self" and "foreign." Introducing immune cells from another person creates several challenges.
First, donor T cells may attack the patient's healthy tissues, causing a potentially dangerous condition called graft-versus-host disease (GvHD).
Second, the patient's immune system may recognize the donor cells as foreign and destroy them before they can eliminate the cancer.
Third, scientists must strike a delicate balance. The engineered cells need to survive long enough to do their job, but not so long that they create new safety concerns.
Remove the native T-cell receptor to reduce the risk of GvHD
Modify immune recognition molecules to make the cells less visible to the patient's immune system
Insert the CAR construct that directs the cells toward cancer
The result is a cell that has been carefully redesigned and programmed for a specific purpose.
Researchers are also exploring additional innovations, including:
Natural killer (NK) cells and γδ T cells, which may have lower risks of immune complications
Built-in safety switches that allow doctors to eliminate the cells if necessary
Logic-gated CARs that activate only when multiple conditions are met, improving precision.
The Manufacturing Challenge
Even if the biology works, another challenge remains: manufacturing. Producing millions or billions of living cells is very different from manufacturing conventional drugs.
Cells change over time. They respond to their environment. Small differences in culture conditions can affect their behavior, potency, and long-term performance.
Researchers must ensure that each batch remains: consistent, potent, stable during freezing and storage and functional after thawing. These are the biggest challenges this field is facing today. The question is no longer just whether we can engineer therapeutic cells. It is whether we can produce them reliably, repeatedly, and at scale.
In many ways, the future of cell therapy depends as much on manufacturing science as it does on molecular biology.
Beyond Cancer: The Future of Living Medicines
Although CAR-T therapy was originally developed to treat cancer, the ideas behind it reach far beyond oncology.
The same technologies that allow scientists to reprogram T cells could eventually be used to create immune cells that treat autoimmune diseases, fight chronic infections, or even act as living sensors that detect disease signals inside the body. Researchers are also exploring synthetic biological circuits that allow cells to sense, process, and respond to changing conditions in real time.
What began as a cancer therapy is increasingly looking like something much bigger: a new class of medicine. Not small molecules. Not antibodies. But living, programmable cells.
The journey is far from over. Important challenges remain, from improving safety and durability to reducing manufacturing costs and ensuring consistent performance across patients. Yet the direction of the field is clear.
For decades, biotechnology focused on discovering drugs that interact with biology. Today, scientists are also learning how to engineer biology itself.
Whether allogeneic CAR-T fully delivers on that promise remains to be seen. But it has already changed how we think about medicine.
Would you like to stay updated on the latest breakthroughs in biomedical science? Subscribe to my blog and join me in exploring the next frontier of medicine!